Eva C. Gombos, MD
Director
At the Division of Breast Imaging, we provide a full range of services for the sophisticated assessment of breast disease and engage in research designed to meet diverse objectives encompassing the modalities available in the Lee Bell Center for Breast Imaging for imaging the anatomy of the breast: Mammography (including Digital Tomosynthesis), Ultrasound, and Magnetic Resonance Imaging (MRI).
We are conducting several retrospective reviews in the Division of Breast Imaging, including a focus on identifying patients who are at high risk for breast cancer in a population with a BRCA1 or BRCA2 altered gene. We are reviewing radiologic-pathologic correlation, an essential component of our clinical breast imaging service. We utilize our research databases to track pathological results and to analyze outcomes. Our specific objectives regarding the concordance of breast imaging and pathology include:
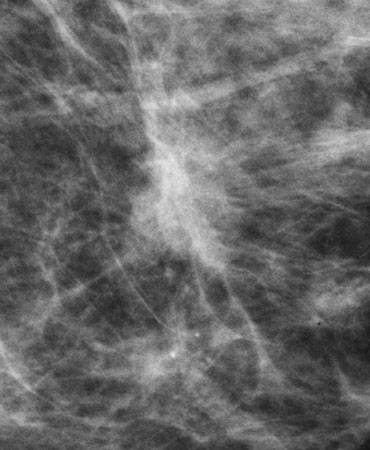
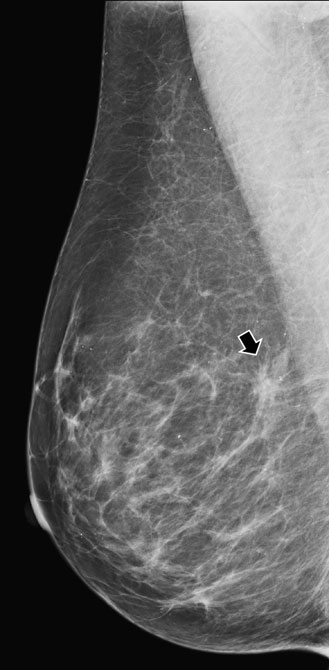 A mammogram (above) showing possible asymmetry, with tomosynthesis images (right) showing superimposed tissue. |
 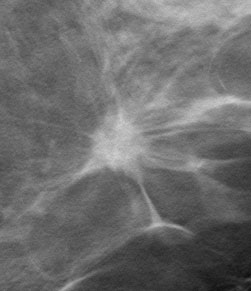 Invasive Ductal Carcinoma on digital mammogram (above left) and digital tomosynthesis (above right). Digital tomosynthesis shows clear presence of a spiculated mass. |
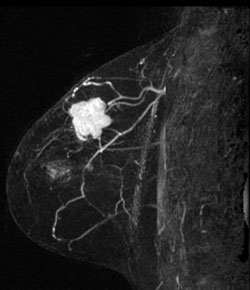
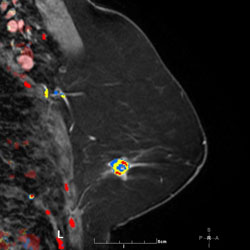 MR Angiomap |
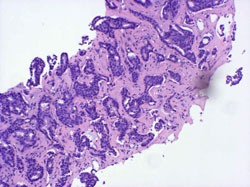 Stereotactic Core Biopsy Histopathology: Infiltrating carcinoma, duct cell type and intraductal carcinoma, cribriform type Grade II. |
A right breast invasive lobular cancer (Estrogen Receptor/Progesterone Receptor +, Her-2 neu -).
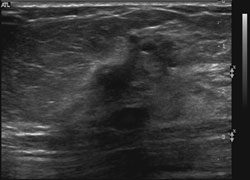 Ultrasound demonstrates a dominant spiculated and irregular hypoechoic mass with dense posterior shadowing (known cancer). There were adjacent, similar-appearing hypoechoic irregular, spiculated masses present also. |
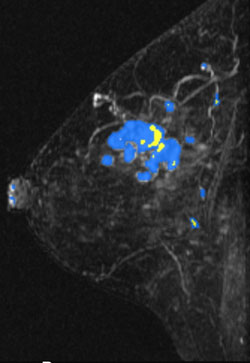 MIP (Maximum Intensity Projection) image of MR shows the known cancer: irregularly marginated mass in the upper outer to central breast. Satellite subcentimeter nodules are present anteromedially and posteriorly. |
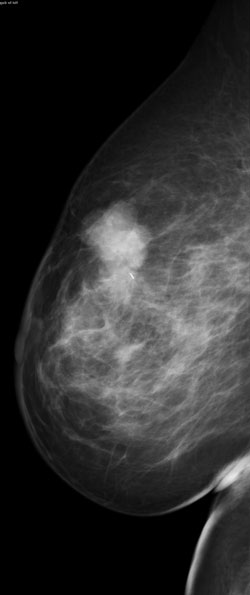 Palpable mass in the upper breast shown on mammography to be irregular. |
 MR MIP image again shows the irregular mass in the upper outer breast. Histology revealed a T2, N0, M0 invasive ductal carcinoma (ER/PR +, Her-2 neu -) and high-grade ductal carcinoma in situ. |
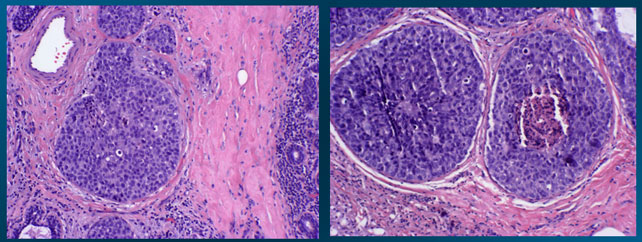 High power view histopathology (H & E) shows high-grade intraductal carcinoma (DCIS). |
For over a century, a leader in patient care, medical education and research, with expertise in virtually every specialty of medicine and surgery.
About BWH

